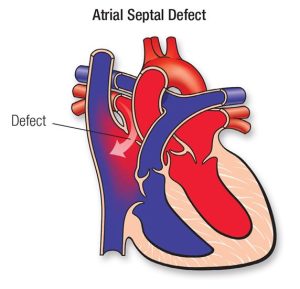
Atrial Septal Defect
A hole between the heart's upper chambers
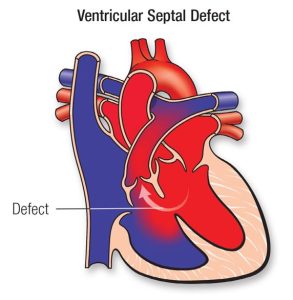
Ventricular Septal Defect
A hole between the heart's lower chambers
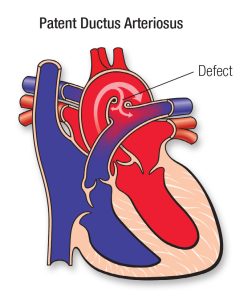
Patent Ductus Arteriosus
A fetal blood vessel that doesn't close after birth
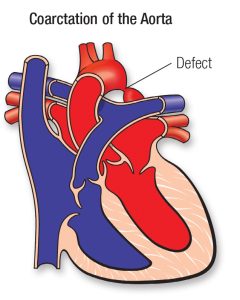
Coarcation of the Aorta
A narrowing of the body's main artery
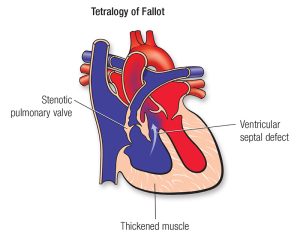
Tetralogy of Fallot
A combination of four heart problems